4.4 Diseases, Disorders and Injuries of the Integumentary System
Learning Objectives
By the end of this section, you will be able to:
- Describe several different diseases and disorders of the skin
- Describe the effect of injury to the skin and the process of healing
The integumentary system is susceptible to a variety of diseases, disorders and injuries. These range from annoying but relatively benign bacterial or fungal infections that are categorised as disorders, to skin cancer and severe burns, which can be fatal. In this section, you will learn several of the most common skin conditions.
Diseases
One of the most talked about diseases is skin cancer. Cancer is a broad term that describes diseases caused by abnormal cells in the body dividing uncontrollably. Most cancers are identified by the organ or tissue in which the cancer originates. One common form of cancer is skin cancer. The Skin Cancer Foundation reports that one in five Americans will experience some type of skin cancer in their lifetime. The degradation of the ozone layer in the atmosphere and the resulting increase in exposure to UV radiation has contributed to its rise. Overexposure to UV radiation damages DNA, which can lead to the formation of cancerous lesions. Although melanin offers some protection against DNA damage from the sun, often it is not enough. The fact that cancers can also occur on areas of the body that are normally not exposed to UV radiation suggests that there are additional factors that can lead to cancerous lesions.
In general, cancers result from an accumulation of DNA mutations. These mutations can result in cell populations that do not die when they should and uncontrolled cell proliferation that leads to tumours. Although many tumours are benign (harmless), some produce cells that can mobilise and establish tumours in other organs of the body; this process is referred to as metastasis. Cancers are characterised by their ability to metastasise.
Basal Cell Carcinoma

Basal cell carcinoma is a form of cancer that affects the mitotically active stem cells in the stratum basale of the epidermis. It is the most common of all cancers that occur in the United States and is frequently found on the head, neck, arms, and back, which are areas that are most susceptible to long-term sun exposure. Although UV rays are the main culprit, exposure to other agents, such as radiation and arsenic, can also lead to this type of cancer. Wounds on the skin due to open sores, tattoos, burns, etc. may be predisposing factors as well. Basal cell carcinomas start in the stratum basale and usually spread along this boundary. At some point, they begin to grow toward the surface and become an uneven patch, bump, growth, or scar on the skin surface (Figure 4.4.1). Like most cancers, basal cell carcinomas respond best to treatment when caught early. Treatment options include surgery, freezing (cryosurgery), and topical ointments (Mayo Clinic 2012).
Squamous Cell Carcinoma

Squamous cell carcinoma is a cancer that affects the keratinocytes of the stratum spinosum and presents as lesions commonly found on the scalp, ears, and hands (Figure 4.4.2). It is the second most common skin cancer. The American Cancer Society reports that two of 10 skin cancers are squamous cell carcinomas, and it is more aggressive than basal cell carcinoma. If not removed, these carcinomas can metastasise. Surgery and radiation are used to cure squamous cell carcinoma.
Melanoma
A melanoma is a cancer characterised by the uncontrolled growth of melanocytes, the pigment-producing cells in the epidermis. Typically, a melanoma develops from a mole. It is the most fatal of all skin cancers, as it is highly metastatic and can be difficult to detect before it has spread to other organs. Melanomas usually appear as asymmetrical brown and black patches with uneven borders and a raised surface (Figure 4.4.3). Treatment typically involves surgical excision and immunotherapy.
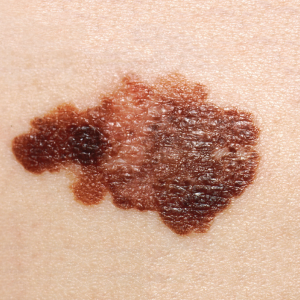
Doctors often give their patients the following ABCDE mnemonic to help with the diagnosis of early-stage melanoma. If you observe a mole on your body displaying these signs, consult a doctor.
Asymmetry – the two sides are not symmetrical
Borders – the edges are irregular in shape
Colour – the colour is varied shades of brown or black
Diameter – it is larger than 6 mm (0.24 in)
Evolving – its shape has changed
Some specialists cite the following additional signs for the most serious form, nodular melanoma:
Elevated – it is raised on the skin surface
Firm – it feels hard to the touch
Growing – it is getting larger
Skin Disorders
Two common skin disorders are eczema and acne. Eczema is an inflammatory condition and occurs in individuals of all ages. Acne involves the clogging of pores, which can lead to infection and inflammation, and is often seen in adolescents. Other disorders, not discussed here, include seborrheic dermatitis (on the scalp), psoriasis, cold sores, impetigo, scabies, hives, and warts.
Eczema

Eczema is an allergic reaction that manifests as dry, itchy patches of skin that resemble rashes (Figure 4.4.4). It may be accompanied by swelling of the skin, flaking, and in severe cases, bleeding. Many who suffer from eczema have antibodies against dust mites in their blood, but the link between eczema and allergy to dust mites has not been proven. Symptoms are usually managed with moisturisers, corticosteroid creams and immunosuppressants.
Acne
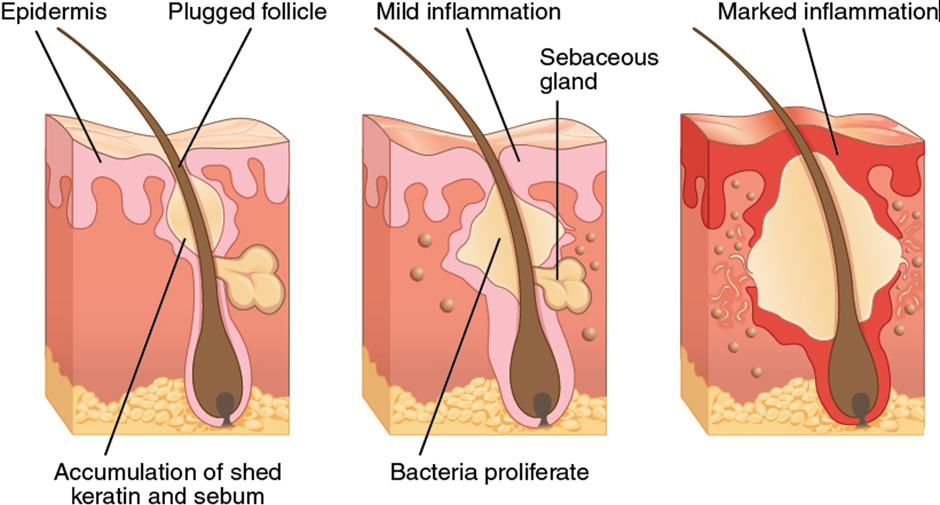
Acne is a skin disturbance that typically occurs on areas of the skin that are rich in sebaceous glands (face and back). It is most common along with the onset of puberty due to associated hormonal changes but can also occur in infants and continue into adulthood. Hormones, such as androgens, stimulate the release of sebum. An overproduction and accumulation of sebum along with keratin can block hair follicles. This plug is initially white. The sebum, when oxidised by exposure to air, turns black. Acne results from infection by acne-causing bacteria (Propionibacterium and Staphylococcus), which can lead to redness and potential scarring due to the natural wound healing process (Figure 4.4.5).
Career Connection
Dermatologist
Have you ever had a skin rash that did not respond to over-the-counter creams, or a mole that you were concerned about? Dermatologists help patients with these types of problems and more, on a daily basis. Dermatologists are medical doctors who specialise in diagnosing and treating skin disorders. Like all medical doctors, dermatologists earn a medical degree and then complete several years of residency training. In addition, dermatologists may then participate in a dermatology fellowship or complete additional, specialised training in a dermatology practice. In Australia, the pathway of becoming a dermatologist has four stages. Firstly, a completion of a medical school degree (medical doctor) which takes roughly four to six years. Second step is a completion of a yearlong in-hospital internship. Third step requires a minimum of one year residency at a hospital. The fourth and final stage requires further vocational training at the Fellowship of the Australasian College of Dermatologists (FACD) for approximately four years.
Most dermatologists work in a medical office or private practice setting. They diagnose skin conditions and rashes, prescribe oral and topical medications to treat skin conditions, and may perform simple procedures, such as mole or wart removal. In addition, they may refer patients to an oncologist if skin cancer that has metastasised is suspected. Recently, cosmetic procedures have also become a prominent part of dermatology. Botox injections, laser treatments, and collagen and dermal filler injections are popular among patients, hoping to reduce the appearance of skin ageing.
Dermatology is a competitive specialty in medicine. Limited openings in dermatology residency programs mean that many medical students compete for a few select spots. Dermatology is an appealing specialty to many prospective doctors, because unlike emergency room physicians or surgeons, dermatologists generally do not have to work excessive hours or be “on-call” weekends and holidays. Moreover, the popularity of cosmetic dermatology has made it a growing field with many lucrative opportunities. It is not unusual for dermatology clinics to market themselves exclusively as cosmetic dermatology centres, and for dermatologists to specialise exclusively in these procedures.
Injuries
Because the skin is the part of our bodies that meets the world most directly, it is especially vulnerable to injury. Injuries include burns and wounds, as well as scars and calluses. They can be caused by sharp objects, heat, or excessive pressure or friction to the skin.
Skin injuries set off a healing process that occurs in several overlapping stages. The first step to repairing damaged skin is the formation of a blood clot that helps stop the flow of blood and scabs over with time. Many different types of cells are involved in wound repair, especially if the surface area that needs repair is extensive. Before the basal stem cells of the stratum basale can recreate the epidermis, fibroblasts mobilise and divide rapidly to repair the damaged tissue by collagen deposition, forming granulation tissue. Blood capillaries follow the fibroblasts and help increase blood circulation and oxygen supply to the area. Immune cells, such as macrophages, roam the area and engulf any foreign matter to reduce the chance of infection.
Burns
A burn results when the skin is damaged by intense heat, radiation, electricity, or chemicals. The damage results in the death of skin cells, which can lead to a massive loss of fluid. Dehydration, electrolyte imbalance, and renal and circulatory failure follow, which can be fatal. Burn patients are treated with intravenous fluids to offset dehydration, as well as intravenous nutrients that enable the body to repair tissues and replace lost proteins. Another serious threat to the lives of burn patients is infection. Burned skin is extremely susceptible to bacteria and other pathogens, due to the loss of protection by intact layers of skin.
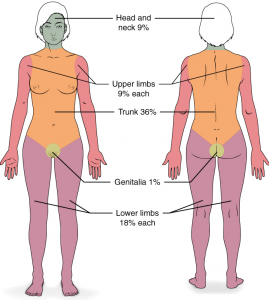
Burns are sometimes measured in terms of the size of the total surface area affected. This is referred to as the “rule of nines”, which associates specific anatomical areas with a percentage that is a factor of nine (Figure 4.4.6). Burns are also classified by the degree of their severity. In Australia, burns are divided into three main categories: superficial, partial thickness, and full thickness. In other countries, such as United States, these are classified by first, second, third and fourth degree burns. Superficial burns (first-degree) appear pink or red in colour with no visible blisters, and only affect the epidermis and dermal papillae. There are no texture changes to the epidermis, however they tend to be hypersensitive to touch. Although the skin may be painful and swollen, these burns typically heal on their own within a few days. Mild sunburn fits into the category of a superficial burn. Partial thickness burns (second-degree), sometimes referred to as mid or deep dermal burns, refer to burns in which the entire epidermal layer had been destroyed and the injury reaches the dermis. The depth to which dermal layer is injured determines whether it is classified as a mid or deep dermal burn. Generally, partial thickness burns are distinguished by a creamy coloured base. In a mid-partial burn, sweat glands and hair follicles remain undamaged, however they are affected in a deep partial thickness burn. These burns result in swelling and a painful blistering of the skin. It is important to keep the burn site clean and sterile to prevent infection. If this is done, the burn will heal within several weeks. Full thickness burns (third-degree) are classified as those in which all layers of the epidermis, epithelial elements, dermal appendages, and nerve endings are injured. These burns are distinguished by a leathery appearance which may range from a white, brown, deep red or black. Additionally, the texture of these layers appears leathery and tough. Full-thickness burns cannot be repaired by the body, because the local tissues used for repair are damaged and require excision (debridement), or amputation in severe cases, followed by grafting of the skin from an unaffected part of the body, or from skin grown in tissue culture for grafting purposes. Oddly, full thickness burns are usually not as painful because the nerve endings themselves are damaged. A fourth-degree burn is even more severe, affecting the underlying muscle and bone.
Scars and Keloids
Most cuts or wounds, with the exception of ones that only scratch the surface (the epidermis), lead to scar formation. A scar is collagen-rich skin formed after the process of wound healing that differs from normal skin. Scarring occurs in cases in which there is repair of skin damage, but the skin fails to regenerate the original skin structure. Fibroblasts generate scar tissue in the form of collagen, and the bulk of repair is due to the basket-weave pattern generated by collagen fibres and does not result in regeneration of the typical cellular structure of skin. Instead, the tissue is fibrous in nature and does not allow for the regeneration of accessory structures, such as hair follicles, sweat glands, or sebaceous glands.
Sometimes, there is an overproduction of scar tissue, because the process of collagen formation does not stop when the wound is healed; this results in the formation of a raised or hypertrophic scar called a keloid. In contrast, scars that result from acne and chickenpox have a sunken appearance and are called atrophic scars.
Scarring of skin after wound healing is a natural process and does not need to be treated further. Application of mineral oil and lotions may reduce the formation of scar tissue. However, modern cosmetic procedures, such as dermabrasion, laser treatments, and filler injections have been invented as remedies for severe scarring. All of these procedures try to reorganise the structure of the epidermis and underlying collagen tissue to make it look more natural.
Bedsores and Stretch Marks
Skin and its underlying tissue can be affected by excessive pressure. One example of this is called a bedsore. Bedsores, also called decubitis ulcers, are caused by constant, long-term, unrelieved pressure on certain body parts that are bony, reducing blood flow to the area and leading to necrosis (tissue death). Bedsores are most common in elderly patients who have debilitating conditions that cause them to be immobile. Most hospitals and long-term care facilities have the practice of turning the patients every few hours to prevent the incidence of bedsores. If left untreated by removal of necrotised tissue, bedsores can be fatal if they become infected.
The skin can also be affected by pressure associated with rapid growth. A stretch mark results when the dermis is stretched beyond its limits of elasticity, as the skin stretches to accommodate the excess pressure. Stretch marks usually accompany rapid weight gain during puberty and pregnancy. They initially have a reddish hue but lighten over time. Other than for cosmetic reasons, treatment of stretch marks is not required. They occur most commonly over the hips and abdomen.
Calluses
When you wear shoes that do not fit well and are a constant source of abrasion on your toes, you tend to form a callus at the point of contact. This occurs because the basal stem cells in the stratum basale are triggered to divide more often to increase the thickness of the skin at the point of abrasion to protect the rest of the body from further damage. This is an example of a minor or local injury, and the skin manages to react and treat the problem independent of the rest of the body. Calluses can also form on your fingers if they are subject to constant mechanical stress, such as long periods of writing, playing string instruments, or video games. A corn is a specialised form of callus. Corns form from abrasions on the skin that result from an elliptical-type motion.
Section Review
Skin cancer is a result of damage to the DNA of skin cells, often due to excessive exposure to UV radiation. Basal cell carcinoma and squamous cell carcinoma are highly curable and arise from cells in the stratum basale and stratum spinosum, respectively. Melanoma is the most dangerous form of skin cancer, affecting melanocytes, which can spread/metastasise to other organs. Burns are an injury to the skin that occur as a result of exposure to extreme heat, radiation, or chemicals. Epidermal, superficial dermal and mid dermal usually heal quickly, but deep dermal and full thickness burns can be fatal because they penetrate the full thickness of the skin. Scars occur when there is repair of skin damage. Fibroblasts generate scar tissue in the form of collagen, which forms a basket-weave pattern that looks different from normal skin.
Bedsores and stretch marks are the result of excessive pressure on the skin and underlying tissue. Bedsores are characterised by necrosis of tissue due to immobility, whereas stretch marks result from rapid growth. Eczema is an allergic reaction that manifests as a rash, and acne results from clogged sebaceous glands. Eczema and acne are usually long-term skin conditions that may be treated successfully in mild cases. Calluses and corns are the result of abrasive pressure on the skin.
Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
