11.4 Bones of the Lower Limb
Learning Objectives
By the end of this section, you will be able to:
- Identify the divisions of the lower limb and describe the bones of each region
- Describe the bones and bony landmarks that articulate at each joint of the lower limb
Like the upper limb, the lower limb is divided into three regions. The thigh is that portion of the lower limb located between the hip joint and knee joint. The leg is specifically the region between the knee joint and the ankle joint. Distal to the ankle is the foot. The lower limb contains 30 bones. These are the femur, patella, tibia, fibula, tarsal bones, metatarsal bones, and phalanges. The femur is the single bone of the thigh. The patella is the kneecap and articulates with the distal femur. The tibia is the larger, weight-bearing bone located on the medial side of the leg, and the fibula is the thin bone of the lateral leg. The bones of the foot are divided into three groups. The posterior portion of the foot is formed by a group of seven bones, each of which is known as a tarsal bone, whereas the mid-foot contains five elongated bones, each of which is a metatarsal bone. The toes contain 14 small bones, each of which is a phalanx bone of the foot.
Femur
The femur, or thigh bone, is the single bone of the thigh region (Figure 11.4.1). It is the longest and strongest bone of the body, and accounts for approximately one-quarter of a person’s total height. The rounded, proximal end is the head of the femur, which articulates with the acetabulum of the hip bone to form the hip joint. The fovea capitis is a minor indentation on the medial side of the femoral head that serves as the site of attachment for the ligament of the head of the femur. This ligament spans the femur and acetabulum but is weak and provides little support for the hip joint. It does, however, carry an important artery that supplies the head of the femur.
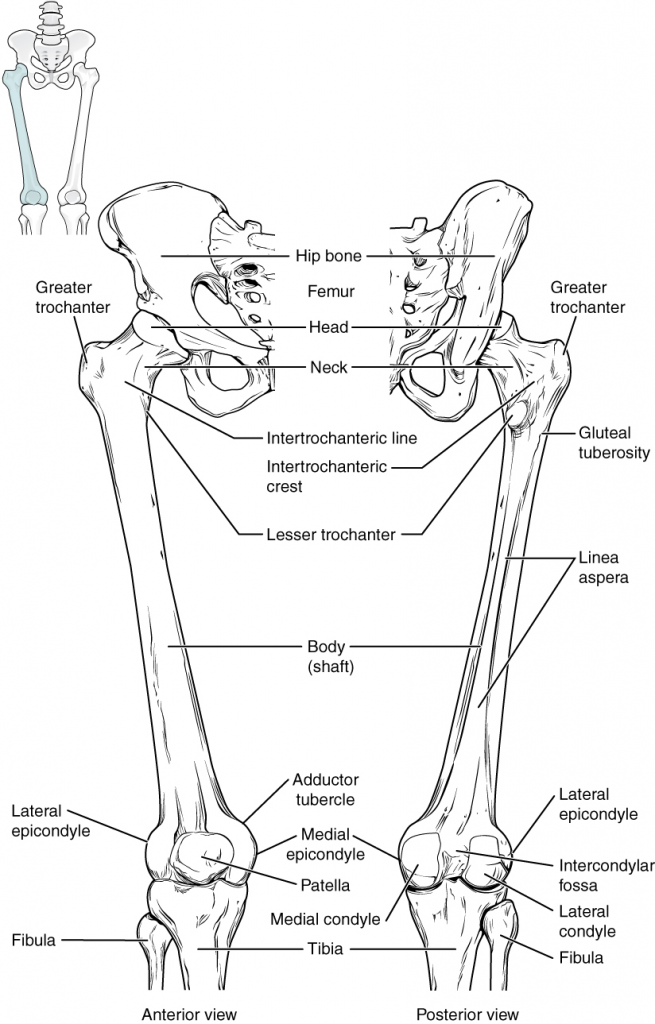
The narrowed region below the head is the neck of the femur. This is a common area for fractures of the femur. The greater trochanter is the large, upward, bony projection located above the base of the neck. Multiple muscles that act across the hip joint attach to the greater trochanter, which, because of its projection from the femur, gives additional leverage to these muscles. The greater trochanter can be felt just under the skin on the lateral side of your upper thigh. The lesser trochanter is a small, bony prominence that lies on the medial aspect of the femur, just below the neck. A single, powerful muscle attaches to the lesser trochanter. Running between the greater and lesser trochanters on the anterior side of the femur is the roughened intertrochanteric line. The trochanters are also connected on the posterior side of the femur by the larger intertrochanteric crest.
The elongated shaft of the femur has a slight anterior bowing or curvature. At its proximal end, the posterior shaft has the gluteal tuberosity, a roughened area extending inferiorly from the greater trochanter. More inferiorly, the gluteal tuberosity becomes continuous with the linea aspera (“rough line”). This is the roughened ridge that passes distally along the posterior side of the mid-femur. Multiple muscles of the hip and thigh regions make long, thin attachments to the femur along the linea aspera.
The distal end of the femur has medial and lateral bony expansions. On the lateral side, the smooth portion that covers the distal and posterior aspects of the lateral expansion is the lateral condyle of the femur. The roughened area on the outer, lateral side of the condyle is the lateral epicondyle of the femur. Similarly, the smooth region of the distal and posterior medial femur is the medial condyle of the femur, and the irregular outer, medial side of this is the medial epicondyle of the femur. The lateral and medial condyles articulate with the tibia to form the knee joint. The epicondyles provide attachment for muscles and supporting ligaments of the knee. The adductor tubercle is a small bump located at the superior margin of the medial epicondyle. Posteriorly, the medial and lateral condyles are separated by a deep depression called the intercondylar fossa. Anteriorly, the smooth surfaces of the condyles join together to form a wide groove called the patellar surface, which provides for articulation with the patella bone. The combination of the medial and lateral condyles with the patellar surface gives the distal end of the femur a horseshoe (U) shape.
Patella
The patella (kneecap) is largest sesamoid bone of the body (see Figure 11.4.1). A sesamoid bone is a bone that is incorporated into the tendon of a muscle where that tendon crosses a joint. The sesamoid bone articulates with the underlying bones to prevent damage to the muscle tendon due to rubbing against the bones during movements of the joint. The patella is found in the tendon of the quadriceps femoris muscle, the large muscle of the anterior thigh that passes across the anterior knee to attach to the tibia. The patella articulates with the patellar surface of the femur and thus prevents rubbing of the muscle tendon against the distal femur. The patella also lifts the tendon away from the knee joint, which increases the leverage power of the quadriceps femoris muscle as it acts across the knee. The patella does not articulate with the tibia.
Homeostatic Imbalances
Runner’s Knee
Runner’s knee, also known as patellofemoral syndrome, is the most common overuse injury among runners. It is most frequent in adolescents and young adults and is more common in females. It often results from excessive running, particularly downhill, but may also occur in athletes who do a lot of knee bending, such as jumpers, skiers, cyclists, weightlifters, and soccer players. It is felt as a dull, aching pain around the front of the knee and deep to the patella. The pain may be felt when walking or running, going up or down stairs, kneeling or squatting, or after sitting with the knee bent for an extended period.
Patellofemoral syndrome may be initiated by a variety of causes, including individual variations in the shape and movement of the patella, a direct blow to the patella, or flat feet or improper shoes that cause excessive turning in or out of the feet or leg. These factors may cause in an imbalance in the muscle pull that acts on the patella, resulting in an abnormal tracking of the patella that allows it to deviate too far toward the lateral side of the patellar surface on the distal femur.
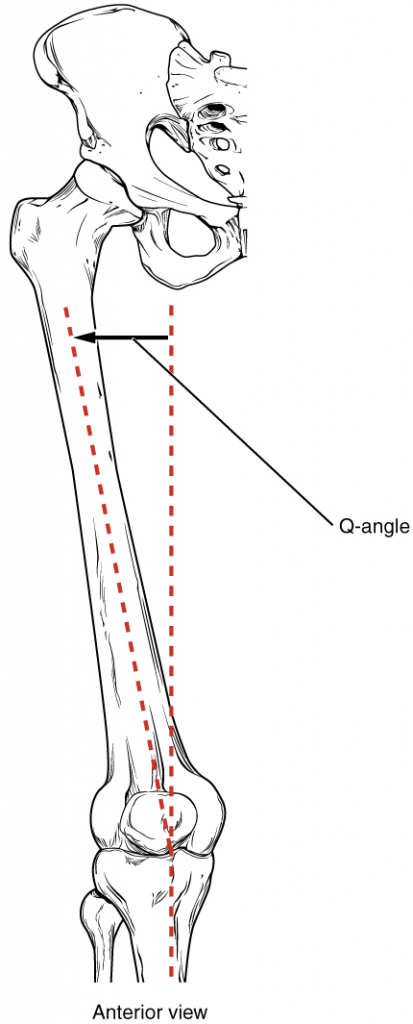
Because the hips are wider than the knee region, the femur has a diagonal orientation within the thigh, in contrast to the vertically oriented tibia of the leg (Figure 11.4.2). The Q-angle is a measure of how far the femur is angled laterally away from vertical. The Q-angle is normally 10–15 degrees, with females typically having a larger Q-angle due to their wider pelvis. During extension of the knee, the quadriceps femoris muscle pulls the patella both superiorly and laterally, with the lateral pull greater in women due to their large Q-angle. This makes women more vulnerable to developing patellofemoral syndrome than men. Normally, the large lip on the lateral side of the patellar surface of the femur compensates for the lateral pull on the patella, and thus helps to maintain its proper tracking.
However, if the pull produced by the medial and lateral sides of the quadriceps femoris muscle is not balanced, abnormal tracking of the patella toward the lateral side may occur. With continued use, this produces pain and could result in damage to the articulating surfaces of the patella and femur, and the potential future development of arthritis. Treatment involves stopping the activity that produces knee pain for a period, followed by a gradual resumption of activity. Proper strengthening of the quadriceps femoris muscle to correct for imbalances is also important to help prevent reoccurrence.
Tibia
The tibia (shin bone) is the medial bone of the leg and is larger than the fibula, with which it is paired (Figure 11.4.3). The tibia is the main weight-bearing bone of the lower leg and the second longest bone of the body, after the femur. The medial side of the tibia is located immediately under the skin, allowing it to be easily palpated down the entire length of the medial leg.
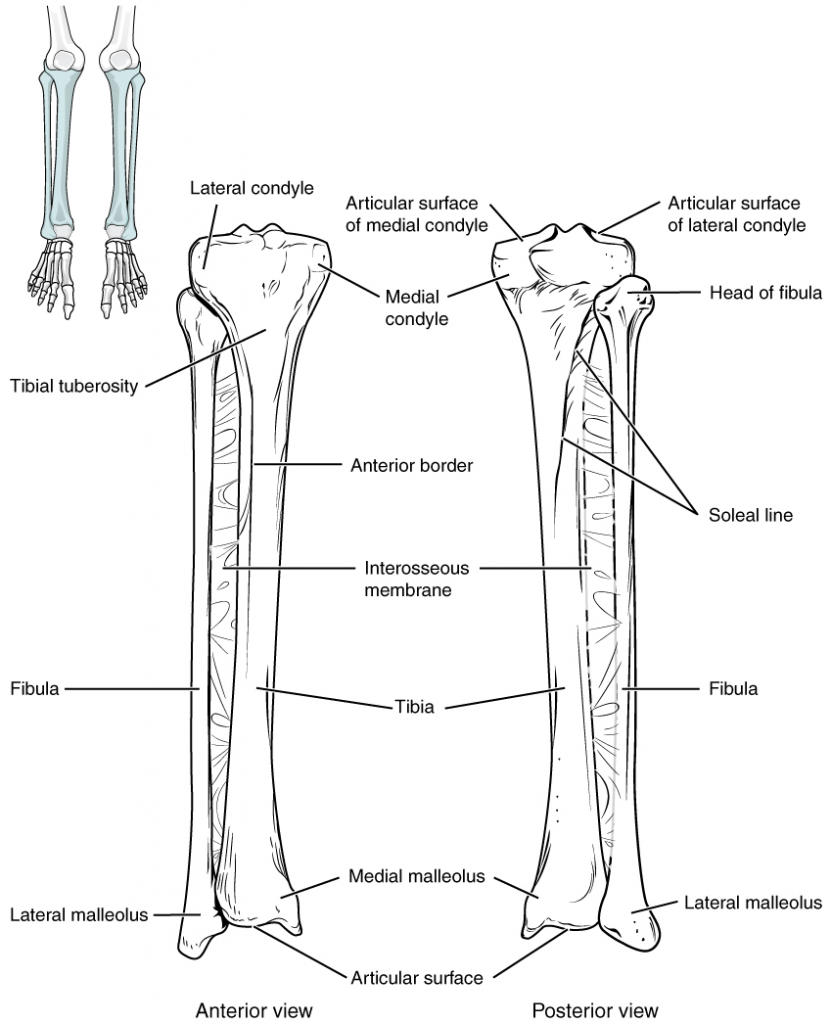
The proximal end of the tibia is greatly expanded. The two sides of this expansion form the medial condyle of the tibia and the lateral condyle of the tibia. The tibia does not have epicondyles. The top surface of each condyle is smooth and flattened. These areas articulate with the medial and lateral condyles of the femur to form the knee joint. Between the articulating surfaces of the tibial condyles is the intercondylar eminence, an irregular, elevated area that serves as the inferior attachment point for two supporting ligaments of the knee.
The tibial tuberosity is an elevated area on the anterior side of the tibia, near its proximal end. It is the final site of attachment for the muscle tendon associated with the patella. More inferiorly, the shaft of the tibia becomes triangular in shape. The anterior apex of
MH this triangle forms the anterior border of the tibia, which begins at the tibial tuberosity and runs inferiorly along the length of the tibia. Both the anterior border and the medial side of the triangular shaft are located immediately under the skin and can be easily palpated along the entire length of the tibia. A small ridge running down the lateral side of the tibial shaft is the interosseous border of the tibia. This is for the attachment of the interosseous membrane of the leg, the sheet of dense connective tissue that unites the tibia and fibula bones. Located on the posterior side of the tibia is the soleal line, a diagonally running, roughened ridge that begins below the base of the lateral condyle, and runs down and medially across the proximal third of the posterior tibia. Muscles of the posterior leg attach to this line.
The large expansion found on the medial side of the distal tibia is the medial malleolus (“little hammer”). This forms the large bony bump found on the medial side of the ankle region. Both the smooth surface on the inside of the medial malleolus and the smooth area at the distal end of the tibia articulate with the talus bone of the foot as part of the ankle joint. On the lateral side of the distal tibia is a wide groove called the fibular notch. This area articulates with the distal end of the fibula, forming the distal tibiofibular joint.
Fibula
The fibula is the slender bone located on the lateral side of the leg (see Figure 11.4.3). The fibula does not bear weight. It serves primarily for muscle attachments and thus is surrounded by muscles. Only the proximal and distal ends of the fibula can be palpated.
The head of the fibula is the small, knob-like, proximal end of the fibula. It articulates with the inferior aspect of the lateral tibial condyle, forming the proximal tibiofibular joint. The thin shaft of the fibula has the interosseous border of the fibula, a narrow ridge running down its medial side for the attachment of the interosseous membrane that spans the fibula and tibia. The distal end of the fibula forms the lateral malleolus, which forms the easily palpated bony bump on the lateral side of the ankle. The deep (medial) side of the lateral malleolus articulates with the talus bone of the foot as part of the ankle joint. The distal fibula also articulates with the fibular notch of the tibia.
Tarsal Bones
The posterior half of the foot is formed by seven tarsal bones (Figure 11.4.4). The most superior bone is the talus. This has a square-shaped upper surface that articulates with the tibia and fibula to form the ankle joint. Three areas of articulation form the ankle joint: The superomedial surface of the talus bone articulates with the medial malleolus of the tibia, the top of the talus articulates with the distal end of the tibia, and the lateral side of the talus articulates with the lateral malleolus of the fibula. Inferiorly, the talus articulates with the calcaneus (heel bone), the largest bone of the foot, which forms the heel. Body weight is transferred from the tibia to the talus to the calcaneus, which rests on the ground. The medial calcaneus has a prominent bony extension called the sustentaculum tali (“support for the talus”) that supports the medial side of the talus bone.
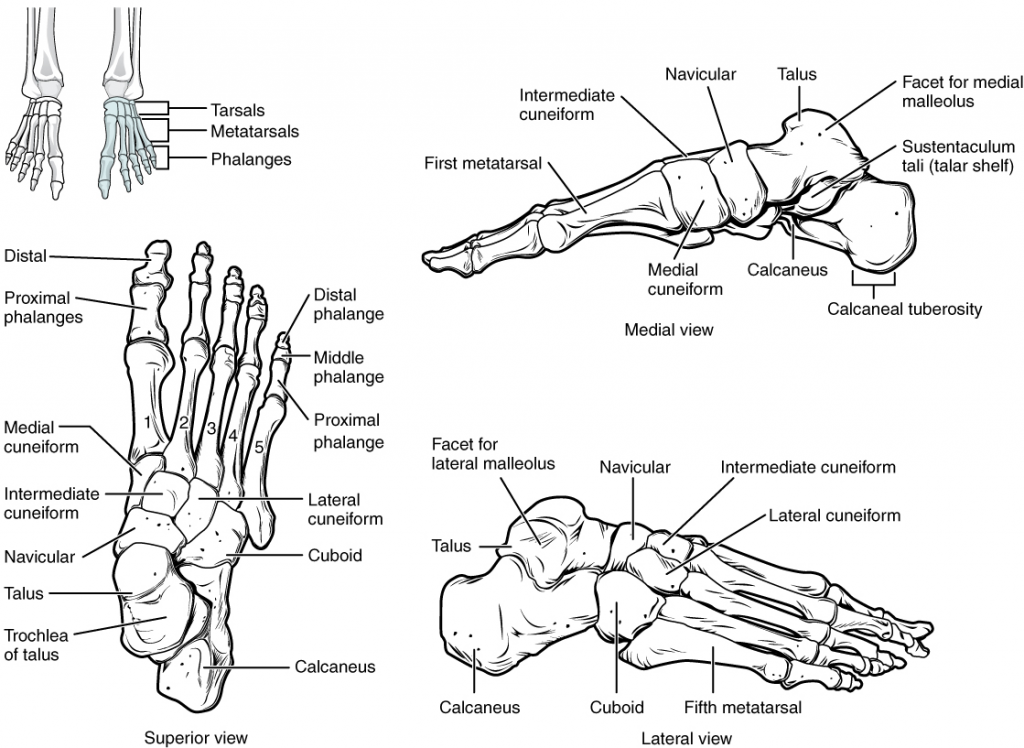
The cuboid bone articulates with the anterior end of the calcaneus bone. The cuboid has a deep groove running across its inferior surface, which provides passage for a muscle tendon. The talus bone articulates anteriorly with the navicular bone, which in turn articulates anteriorly with the three cuneiform (“wedge-shaped”) bones. These bones are the medial cuneiform, the intermediate cuneiform, and the lateral cuneiform. Each of these bones has a broad superior surface and a narrow inferior surface, which together produce the transverse (medial-lateral) curvature of the foot. The navicular and lateral cuneiform bones also articulate with the medial side of the cuboid bone.
Metatarsal Bones
The anterior half of the foot is formed by the five metatarsal bones, which are located between the tarsal bones of the posterior foot and the phalanges of the toes (see Figure 11.4.4). These elongated bones are numbered 1–5, starting with the medial side of the foot. The first metatarsal bone is shorter and thicker than the others. The second metatarsal is the longest. The base of the metatarsal bone is the proximal end of each metatarsal bone. These articulate with the cuboid or cuneiform bones. The base of the fifth metatarsal has a large, lateral expansion that provides for muscle attachments. This expanded base of the fifth metatarsal can be felt as a bony bump at the midpoint along the lateral border of the foot. The expanded distal end of each metatarsal is the head of the metatarsal bone. Each metatarsal bone articulates with the proximal phalanx of a toe to form a metatarsophalangeal joint. The heads of the metatarsal bones also rest on the ground and form the ball (anterior end) of the foot.
Phalanges
The toes contain a total of 14 phalanx bones (phalanges), arranged in a similar manner as the phalanges of the fingers (see Figure 11.4.4). The toes are numbered 1–5, starting with the big toe (hallux). The big toe has two phalanx bones, the proximal and distal phalanges. The remaining toes all have proximal, middle, and distal phalanges. A joint between adjacent phalanx bones is called an interphalangeal joint.
Arches of the Foot
When the foot meets the ground during walking, running, or jumping activities, the impact of the body weight puts a tremendous amount of pressure and force on the foot. During running, the force applied to each foot as it contacts the ground can be up to 2.5 times your body weight. The bones, joints, ligaments, and muscles of the foot absorb this force, thus greatly reducing the amount of shock that is passed superiorly into the lower limb and body. The arches of the foot play a key role in this shock-absorbing ability. When weight is applied to the foot, these arches will flatten, thus absorbing energy. When the weight is removed, the arch rebounds, giving “spring” to the step. The arches also serve to distribute body weight side to side and to either end of the foot.
The foot has a transverse arch, a medial longitudinal arch, and a lateral longitudinal arch (see Figure 11.4.4). The transverse arch forms the medial-lateral curvature of the mid-foot. It is formed by the wedge shapes of the cuneiform bones and bases (proximal ends) of the first to fourth metatarsal bones. This arch helps to distribute body weight from side to side within the foot, thus allowing the foot to accommodate uneven terrain.
The longitudinal arches run down the length of the foot. The lateral longitudinal arch is flat, whereas the medial longitudinal arch is larger (taller). The longitudinal arches are formed by the tarsal bones posteriorly and the metatarsal bones anteriorly. These arches are supported at either end, where they contact the ground. Posteriorly, this support is provided by the calcaneus bone and anteriorly by the heads (distal ends) of the metatarsal bones. The talus bone, which receives the weight of the body, is located at the top of the longitudinal arches. Body weight is then conveyed from the talus to the ground by the anterior and posterior ends of these arches. Strong ligaments unite the adjacent foot bones to prevent disruption of the arches during weight bearing. On the bottom of the foot, additional ligaments tie together the anterior and posterior ends of the arches. These ligaments have elasticity, which allows them to stretch during weight bearing, thus allowing the longitudinal arches to spread. The stretching of these ligaments stores energy within the foot, rather than passing these forces into the leg. Contraction of the foot muscles also plays a key role in this energy absorption. When the weight is removed, the elastic ligaments recoil and pull the ends of the arches closer together. This recovery of the arches releases the stored energy and improves the energy efficiency of walking.
Stretching of the ligaments that support the longitudinal arches can lead to pain. This can occur in overweight individuals, with people who have jobs that involve standing for extended periods of time (such as wait-staff) or walking or running long distances. If stretching of the ligaments is prolonged, excessive, or repeated, it can result in a gradual lengthening of the supporting ligaments, with subsequent depression or collapse of the longitudinal arches, particularly on the medial side of the foot. This condition is called pes planus (“flat foot” or “fallen arches”).
Section Review
The lower limb is divided into three regions. These are the thigh, located between the hip and knee joints; the leg, located between the knee and ankle joints; and distal to the ankle, the foot. There are 30 bones in each lower limb. These are the femur, patella, tibia, fibula, seven tarsal bones, five metatarsal bones, and 14 phalanges.
The femur is the single bone of the thigh. Its rounded head articulates with the acetabulum of the hip bone to form the hip joint. The head has the fovea capitis for attachment of the ligament of the head of the femur. The narrow neck joins inferiorly with the greater and lesser trochanters. Passing between these bony expansions are the intertrochanteric line on the anterior femur and the larger intertrochanteric crest on the posterior femur. On the posterior shaft of the femur is the gluteal tuberosity proximally and the linea aspera in the mid-shaft region. The expanded distal end consists of three articulating surfaces: the medial and lateral condyles, and the patellar surface. The outside margins of the condyles are the medial and lateral epicondyles. The adductor tubercle is on the superior aspect of the medial epicondyle.
The patella is a sesamoid bone located within a muscle tendon. It articulates with the patellar surface on the anterior side of the distal femur, thereby protecting the muscle tendon from rubbing against the femur.
The leg contains the large tibia on the medial side and the slender fibula on the lateral side. The tibia bears the weight of the body, whereas the fibula does not bear weight. The interosseous border of each bone is the attachment site for the interosseous membrane of the leg, the connective tissue sheet that unites the tibia and fibula.
The proximal tibia consists of the expanded medial and lateral condyles, which articulate with the medial and lateral condyles of the femur to form the knee joint. Between the tibial condyles is the intercondylar eminence. On the anterior side of the proximal tibia is the tibial tuberosity, which is continuous inferiorly with the anterior border of the tibia. On the posterior side, the proximal tibia has the curved soleal line. The bony expansion on the medial side of the distal tibia is the medial malleolus. The groove on the lateral side of the distal tibia is the fibular notch.
The head of the fibula forms the proximal end and articulates with the underside of the lateral condyle of the tibia. The distal fibula articulates with the fibular notch of the tibia. The expanded distal end of the fibula is the lateral malleolus.
The posterior foot is formed by the seven tarsal bones. The talus articulates superiorly with the distal tibia, the medial malleolus of the tibia, and the lateral malleolus of the fibula to form the ankle joint. The talus articulates inferiorly with the calcaneus bone. The sustentaculum tali of the calcaneus helps to support the talus. Anterior to the talus is the navicular bone, and anterior to this are the medial, intermediate, and lateral cuneiform bones. The cuboid bone is anterior to the calcaneus.
The five metatarsal bones form the anterior foot. The base of these bones articulates with the cuboid or cuneiform bones. The metatarsal heads, at their distal ends, articulate with the proximal phalanges of the toes. The big toe (toe number 1) has proximal and distal phalanx bones. The remaining toes have proximal, middle, and distal phalanges.
Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
