12.1 Overview of the Digestive System
Learning Objectives
By the end of this section, you will be able to:
- Identify the organs of the gastrointestinal tract (alimentary canal) from proximal to distal, and briefly state their function
- Identify the accessory digestive organs and briefly state their function
- Describe the four fundamental tissue layers of the gastrointestinal tract
- Contrast the contributions of the enteric and autonomic nervous systems to digestive system functioning
- Explain how the peritoneum anchors the digestive organs
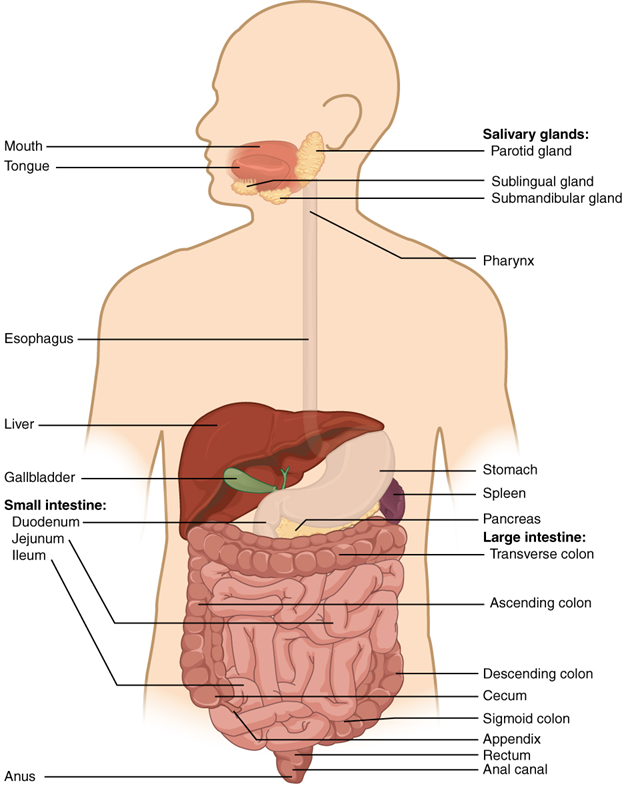
The function of the digestive system is to break down the foods you eat, release their nutrients, and absorb those nutrients into the body. Although the small intestine is the workhorse of the system, where the majority of digestion occurs, and where most of the released nutrients are absorbed into the blood or lymph, each of the digestive system organs makes a vital contribution to this process (Figure 12.1.1).
As is the case with all body systems, the digestive system does not work in isolation; it functions cooperatively with the other systems of the body. Consider for example, the interrelationship between the digestive and cardiovascular systems. Arteries supply the digestive organs with oxygen and processed nutrients, and veins drain the digestive tract. These intestinal veins, constituting the hepatic portal system, are unique; they do not return blood directly to the heart. Rather, this blood is diverted to the liver where its nutrients are off-loaded for processing before blood completes its circuit back to the heart. At the same time, the digestive system provides nutrients to the heart muscle and vascular tissue to support their functioning. The interrelationship of the digestive and endocrine systems is also critical. Hormones secreted by several endocrine glands, as well as endocrine cells of the pancreas, the stomach, and the small intestine, contribute to the control of digestion and nutrient metabolism. In turn, the digestive system provides the nutrients to fuel endocrine function. Table 12.1.1 gives a quick glimpse at how these other systems contribute to the functioning of the digestive system.
Table 12.1.1. Contribution of Other Body Systems to the Digestive System
| Body system | Benefits received by the digestive system |
| Cardiovascular | Blood supplies digestive organs with oxygen and processed nutrients |
| Endocrine | Endocrine hormones help regulate secretion in digestive glands and accessory organs
|
| Integumentary | Skin helps protect digestive organs and synthesises vitamin D for calcium absorption
|
| Lymphatic | Mucosa-associated lymphoid tissue and other lymphatic tissue defend against entry of pathogens; lacteal absorb lipids; and lymphatic vessels transport lipids to bloodstream
|
| Muscular | Skeletal muscles support and protect abdominal organs |
| Nervous | Sensory and motor neurons help regulate secretions and muscle contractions in the digestive tract
|
| Respiratory | Respiratory organs provide oxygen and remove carbon dioxide |
| Skeletal | Bones help protect and support digestive organs |
| Urinary | Kidneys convert vitamin D into its active form, allowing calcium absorption in the small intestine |
Digestive System Organs
The easiest way to understand the digestive system is to divide its organs into two main categories. The first group is the organs that make up the gastrointestinal tract. Accessory digestive organs comprise the second group and are critical for orchestrating the breakdown of food and the assimilation of its nutrients into the body. Accessory digestive organs, despite their name, are critical to the function of the digestive system.
Gastrointestinal Tract Organs
Also called the gastrointestinal (GI) tract or gut, the gastrointestinal tract (aliment- = “to nourish”) is a hollow, muscular, one-way tube about 7.62 metres in length during life and closer to 10.67 metres in length when measured after death, once smooth muscle tone is lost. The main function of the organs of the gastrointestinal tract is to nourish the body. This tube begins at the mouth and terminates at the anus. Between those two points, the canal is modified as the pharynx, oesophagus, stomach, and small and large intestines to fit the functional needs of the body. Both the mouth and anus are open to the external environment; thus, food and wastes within the gastrointestinal tract are technically considered to be outside the body. Only through the process of absorption do the nutrients in food enter into and nourish the body’s “inner space.”
Accessory Structures
Each accessory digestive organ aids in the breakdown of food (Figure 12.1.2). Within the mouth, the teeth and tongue begin mechanical digestion, whereas the salivary glands begin chemical digestion. Once food products enter the small intestine, the gallbladder, liver, and pancreas release secretions—such as bile and enzymes—essential for digestion to continue. Together, these are called accessory organs because they sprout from the lining cells of the developing gut (mucosa) and augment its function; indeed, you could not live without their vital contributions, and many significant diseases result from their malfunction. Even after development is complete, they maintain a connection to the gut by way of ducts.
Histology of the Gastrointestinal Tract
Throughout its length, the alimentary tract is composed of the same four tissue layers; the details of their structural arrangements vary to fit their specific functions. Starting from the lumen and moving outwards, these layers are the mucosa, submucosa, muscularis, and serosa, which is continuous with the mesentery (see Figure 12.1.2).
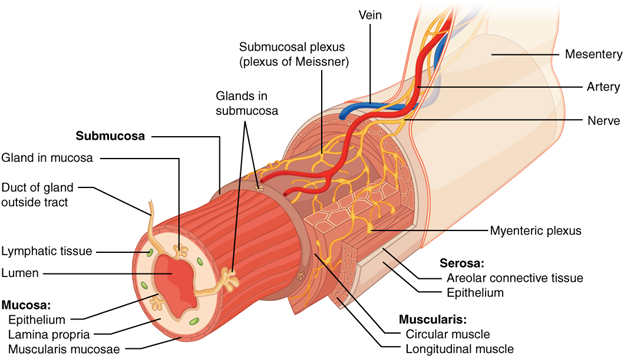
The mucosa is referred to as a mucous membrane, because mucus production is a characteristic feature of gut epithelium. The membrane consists of epithelium, which is in direct contact with ingested food, and the lamina propria, a layer of connective tissue analogous to the dermis. In addition, the mucosa has a thin, smooth muscle layer, called the muscularis mucosa (not to be confused with the muscularis layer, described below).
Epithelium—In the mouth, pharynx, oesophagus, and anal canal, the epithelium is primarily a non-keratinised, stratified squamous epithelium. In the stomach and intestines, it is a simple columnar epithelium. Notice that the epithelium is in direct contact with the lumen, the space inside the gastrointestinal tract. Interspersed among its epithelial cells are goblet cells, which secrete mucus and fluid into the lumen, and enteroendocrine cells, which secrete hormones into the interstitial spaces between cells. Epithelial cells have a very brief lifespan, averaging from only a couple of days (in the mouth) to about a week (in the gut). This process of rapid renewal helps preserve the health of the gastrointestinal tract, despite the wear and tear resulting from continued contact with foodstuffs.
Lamina propria—In addition to loose connective tissue, the lamina propria contains numerous blood and lymphatic vessels that transport nutrients absorbed through the gastrointestinal tract to other parts of the body. The lamina propria also serves an immune function by housing clusters of lymphocytes, making up the mucosa-associated lymphoid tissue (MALT). These lymphocyte clusters are particularly substantial in the distal ileum where they are known as Peyer’s patches. When you consider that the gastrointestinal tract is exposed to foodborne bacteria and other foreign matter, it is not hard to appreciate why the immune system has evolved a means of defending against the pathogens encountered within it.
Muscularis mucosa—This thin layer of smooth muscle is in a constant state of tension, pulling the mucosa of the stomach and small intestine into undulating folds. These folds dramatically increase the surface area available for digestion and absorption.
As its name implies, the submucosa lies immediately beneath the mucosa. A broad layer of dense connective tissue, it connects the overlying mucosa to the underlying muscularis. It includes blood and lymphatic vessels (which transport absorbed nutrients), and a scattering of submucosal glands that release digestive secretions. Additionally, it serves as a conduit for a dense branching network of nerves, the submucosal plexus, which functions as described below.
The third layer of the gastrointestinal tract is the muscularis (also called the muscularis externa). The muscularis in the small intestine is made up of a double layer of smooth muscle: an inner circular layer and an outer longitudinal layer. The contractions of these layers promote mechanical digestion, expose more of the food to digestive chemicals, and move the food along the canal. In the most proximal and distal regions of the gastrointestinal tract, including the mouth, pharynx, anterior part of the oesophagus, and external anal sphincter, the muscularis is made up of skeletal muscle, which gives you voluntary control over swallowing and defecation. The basic two-layer structure found in the small intestine is modified in the organs proximal and distal to it. The stomach is equipped for its churning function by the addition of a third layer, the oblique muscle. While the colon has two layers like the small intestine, its longitudinal layer is segregated into three narrow parallel bands, the taeniae coli, which make it look like a series of pouches rather than a simple tube.
The serosa is the portion of the gastrointestinal tract superficial to the muscularis. Present only in the region of the gastrointestinal tract within the abdominal cavity, it consists of a layer of visceral peritoneum overlying a layer of loose connective tissue. Instead of serosa, the mouth, pharynx, and oesophagus have a dense sheath of collagen fibres called the adventitia. These tissues serve to hold the gastrointestinal tract in place near the ventral surface of the vertebral column.
Nerve Supply
As soon as food enters the mouth, it is detected by receptors that send impulses along the sensory neurons of cranial nerves. Without these nerves, not only would your food be without taste, but you would also be unable to feel either the food or the structures of your mouth, and you would be unable to avoid biting yourself as you chew, an action enabled by the motor branches of cranial nerves.
Intrinsic innervation of much of the gastrointestinal tract is provided by the enteric nervous system, which runs from the oesophagus to the anus, and contains approximately 100 million motor, sensory, and interneurons (unique to this system compared to all other parts of the peripheral nervous system). These enteric neurons are grouped into two plexuses. The myenteric plexus (plexus of Auerbach) lies in the muscularis layer of the gastrointestinal tract and is responsible for motility, especially the rhythm and force of the contractions of the muscularis. The submucosal plexus (plexus of Meissner) lies in the submucosal layer and is responsible for regulating digestive secretions and reacting to the presence of food.
Extrinsic innervations of the gastrointestinal tract are provided by the autonomic nervous system, which includes both sympathetic and parasympathetic nerves. In general, sympathetic activation (the fight-or-flight response) restricts the activity of enteric neurons, thereby decreasing GI secretion and motility. In contrast, parasympathetic activation (the rest-and-digest response) increases GI secretion and motility by stimulating neurons of the enteric nervous system.
Blood Supply
The blood vessels serving the digestive system have two functions. They transport the protein and carbohydrate nutrients absorbed by mucosal cells after food is digested in the lumen. Lipids are absorbed via lacteals, tiny structures of the lymphatic system. The blood vessels’ second function is to supply the organs of the gastrointestinal tract with the nutrients and oxygen needed to drive their cellular processes.
Specifically, the more anterior parts of the gastrointestinal tract are supplied with blood by arteries branching off the aortic arch and thoracic aorta. Below this point, the gastrointestinal tract is supplied with blood by arteries branching from the abdominal aorta. The celiac trunk services the liver, stomach, and duodenum, whereas the superior and inferior mesenteric arteries supply blood to the remaining small and large intestines.
The veins that collect nutrient-rich blood from the small intestine (where most absorption occurs) empty into the hepatic portal system. This venous network takes the blood into the liver where the nutrients are either processed or stored for later use. Only then does the blood drained from the gastrointestinal tract viscera circulate back to the heart. To appreciate just how demanding the digestive process is on the cardiovascular system, consider that while you are “resting and digesting,” about one-fourth of the blood pumped with each heartbeat enters arteries serving the intestines.
The Peritoneum
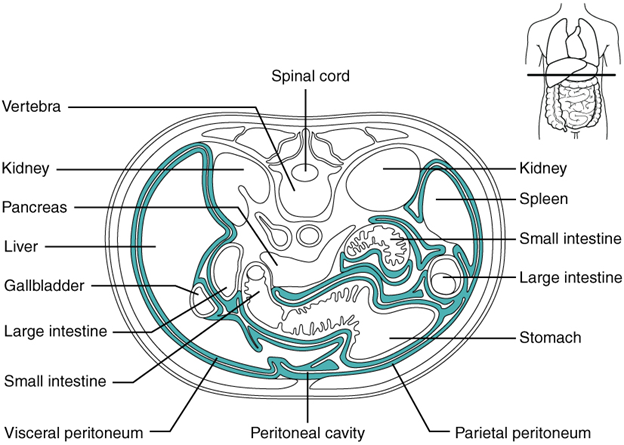
The digestive organs within the abdominal cavity are held in place by the peritoneum, a broad serous membranous sac made up of squamous epithelial tissue surrounded by connective tissue. It is composed of two different regions: the parietal peritoneum, which lines the abdominal wall, and the visceral peritoneum, which envelopes the abdominal organs (Figure 12.1.3). The peritoneal cavity is the space bounded by the visceral and parietal peritoneal surfaces. A few millilitres of watery fluid act as a lubricant to minimise friction between the serosal surfaces of the peritoneum.
Disorders of the Digestive System: Peritonitis
Inflammation of the peritoneum is called peritonitis. Chemical peritonitis can develop any time the wall of the gastrointestinal tract is breached, allowing the contents of the lumen entry into the peritoneal cavity, for example, when an ulcer perforates the stomach wall, gastric juices spill into the peritoneal cavity. Haemorrhagic peritonitis occurs after a ruptured tubal pregnancy or traumatic injury to the liver or spleen fills the peritoneal cavity with blood. Even more severe peritonitis is associated with bacterial infections seen with appendicitis, colonic diverticulitis, and pelvic inflammatory disease (infection of uterine tubes, usually by sexually transmitted bacteria). Peritonitis is life threatening and often results in emergency surgery to correct the underlying problem and intensive antibiotic therapy. When your great grandparents and even your parents were young, the mortality from peritonitis was high. Aggressive surgery, improvements in anaesthesia safety, the advance of critical care expertise, and antibiotics have greatly improved the mortality rate from this condition. Even so, the mortality rate still ranges from 30 to 40 percent.
The visceral peritoneum includes multiple large folds that envelope various abdominal organs, holding them to the dorsal surface of the body wall. Within these folds are blood vessels, lymphatic vessels, and nerves that innervate the organs with which they are in contact, supplying their adjacent organs. The five major peritoneal folds are described in Table 12.1.2. Note that during foetal development, certain digestive structures, including the first portion of the small intestine (called the duodenum), the pancreas, and portions of the large intestine (the ascending and descending colon, and the rectum) remain completely or partially posterior to the peritoneum. Thus, the location of these organs is described as retroperitoneal.
Table 12.1.2. The Five Major Peritoneal Folds
| Fold | Description |
| Greater omentum | Apron-like structure that lies superficial to the small intestine and transverse colon; a site of fat deposition in people who are overweight
|
| Falciform ligament | Anchors the liver to the anterior abdominal wall and inferior border of the diaphragm
|
| Lesser omentum | Suspends the stomach from the inferior border of the liver; provides a pathway for structures connecting to the liver
|
| Mesentery | Vertical band of tissue anterior to the lumbar vertebrae and anchoring all of the small intestine except the initial portion (the duodenum)
|
| Mesocolon | Attaches two portions of the large intestine (the transverse and sigmoid colon) to the posterior abdominal wall |
Section Review
The digestive system includes the organs of the gastrointestinal tract and accessory structures. The gastrointestinal tract forms a continuous tube that is open to the outside environment at both ends. The organs of the gastrointestinal tract are the mouth, pharynx, oesophagus, stomach, small intestine, and large intestine. The accessory digestive structures include the teeth, tongue, salivary glands, liver, pancreas and gallbladder. The wall of the gastrointestinal tract is composed of four basic tissue layers: mucosa, submucosa, muscularis and serosa. The enteric nervous system provides intrinsic innervation, and the autonomic nervous system provides extrinsic innervation.
Section Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
