12.3 The Mouth, Pharynx and Oesophagus
Learning Objectives
By the end of this section, you will be able to:
- Describe the structures of the mouth, including its three accessory digestive organs
- Group the 32 adult teeth according to name, location, and function
- Describe the process of swallowing, including the roles of the tongue, upper oesophageal sphincter and epiglottis
- Trace the pathway food follows from ingestion into the mouth through release into the stomach
In this section, you will examine the anatomy and functions of the three main organs of the upper gastrointestinal tract—the mouth, pharynx, and oesophagus—as well as three associated accessory organs—the tongue, salivary glands and teeth.
The Mouth
The cheeks, tongue, and palate frame the mouth, which is also called the oral cavity (or buccal cavity). The structures of the mouth are illustrated in Figure 12.3.1.
At the entrance to the mouth are the lips, or labia (singular = labium). Their outer covering is skin, which transitions to a mucous membrane in the mouth proper. Lips are very vascular with a thin layer of keratin; hence, the reason they are “red.” They have a huge representation on the cerebral cortex, which probably explains the human fascination with kissing! The lips cover the orbicularis oris muscle, which regulates what comes in and goes out of the mouth. The labial frenulum is a midline fold of mucous membrane that attaches the inner surface of each lip to the gum. The cheeks make up the oral cavity’s sidewalls. While their outer covering is skin, their inner covering is mucous membrane. This membrane is made up of non-keratinised, stratified squamous epithelium. Between the skin and mucous membranes are connective tissue and buccinator muscles. The next time you eat some food, notice how the buccinator muscles in your cheeks and the orbicularis oris muscle in your lips contract, helping you keep the food from falling out of your mouth. Additionally, notice how these muscles work when you are speaking.
The pocket-like part of the mouth that is framed on the inside by the gums and teeth, and on the outside by the cheeks and lips is called the oral vestibule. Moving farther into the mouth, the opening between the oral cavity and throat (oropharynx) is called the fauces (like the kitchen “faucet”). The main open area of the mouth, or oral cavity proper, runs from the gums and teeth to the fauces.
When you are chewing, you do not find it difficult to breathe simultaneously. The next time you have food in your mouth, notice how the arched shape of the roof of your mouth allows you to handle both digestion and respiration at the same time. This arch is called the palate. The anterior region of the palate serves as a wall (or septum) between the oral and nasal cavities as well as a rigid shelf against which the tongue can push food. It is created by the maxillary and palatine bones of the skull and, given its bony structure, is known as the hard palate. If you run your tongue along the roof of your mouth, you’ll notice that the hard palate ends in the posterior oral cavity, and the tissue becomes fleshier. This part of the palate, known as the soft palate, is composed mainly of skeletal muscle. You can therefore manipulate, subconsciously, the soft palate—for instance, to yawn, swallow, or sing (see Figure 12.3.1).
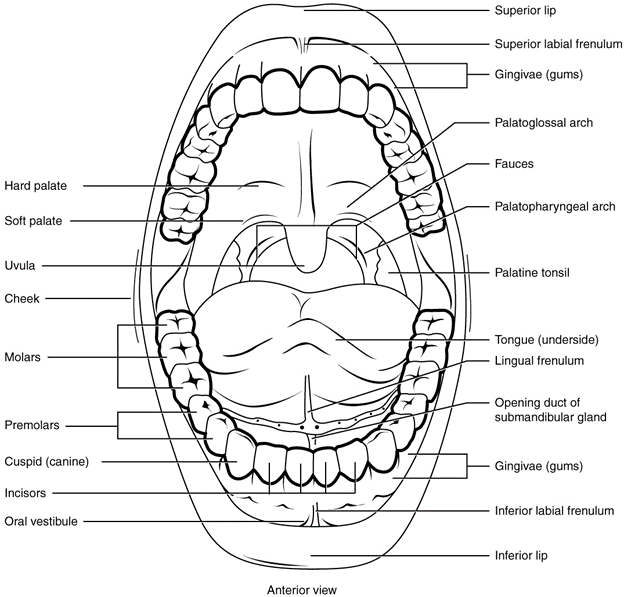
A fleshy bead of tissue called the uvula drops down from the centre of the posterior edge of the soft palate. Although some have suggested that the uvula is a vestigial organ, it serves an important purpose. When you swallow, the soft palate and uvula move upward, helping to keep foods and liquid from entering the nasal cavity. Unfortunately, it can also contribute to the sound produced by snoring. Two muscular folds extend downward from the soft palate, on either side of the uvula. Toward the front, the palatoglossal arch lies next to the base of the tongue; behind it, the palatopharyngeal arch forms the superior and lateral margins of the fauces. Between these two arches are the palatine tonsils, clusters of lymphoid tissue that protect the pharynx. The lingual tonsils are located at the base of the tongue.
The Tongue
Perhaps you have heard it said that the tongue is the strongest muscle in the body. Those who stake this claim cite its strength proportionate to its size. Although it is difficult to quantify the relative strength of different muscles, it remains indisputable that the tongue is a workhorse, facilitating ingestion, mechanical digestion, chemical digestion (lingual lipase), sensation (of taste, texture, and temperature of food), swallowing, and vocalisation.
The tongue is attached to the mandible, the styloid processes of the temporal bones, and the hyoid bone. The hyoid is unique in that it only distantly/indirectly articulates with other bones. The tongue is positioned over the floor of the oral cavity. A medial septum extends the entire length of the tongue, dividing it into symmetrical halves.
Beneath its mucous membrane covering, each half of the tongue is composed of the same number and type of intrinsic and extrinsic skeletal muscles. The intrinsic muscles (those within the tongue) are the longitudinalis inferior, longitudinalis superior, transversus linguae, and verticalis linguae muscles. These allow you to change the size and shape of your tongue, as well as to stick it out, if you wish. Having such a flexible tongue facilitates both swallowing and speech.
As you learned in your study of the muscular system, the extrinsic muscles of the tongue are the mylohyoid, hyoglossus, styloglossus, and genioglossus muscles. These muscles originate outside the tongue and insert into connective tissues within the tongue. The mylohyoid is responsible for raising the tongue, the hyoglossus pulls it down and back, the styloglossus pulls it up and back, and the genioglossus pulls it forward. Working in concert, these muscles perform three important digestive functions in the mouth: (1) position food for optimal chewing, (2) gather food into a bolus (rounded mass), and (3) position food so it can be swallowed.
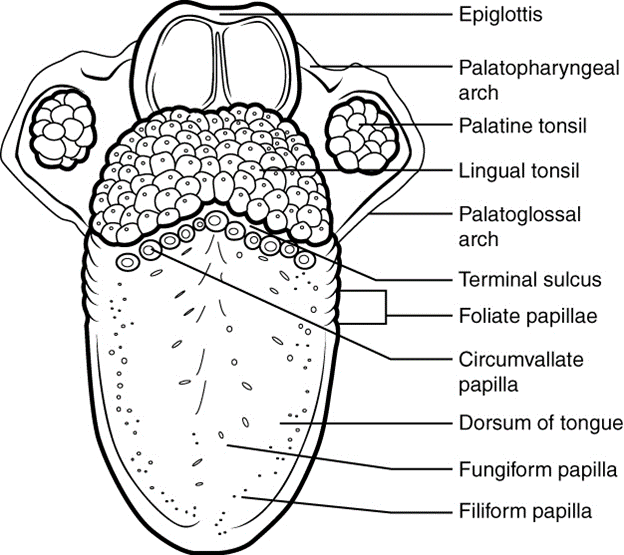
The top and sides of the tongue are studded with papillae, extensions of lamina propria of the mucosa, which are covered in stratified squamous epithelium (Figure 12.3.2). Fungiform papillae, which are mushroom shaped, cover a large area of the tongue; they tend to be larger toward the rear of the tongue and smaller on the tip and sides. In contrast, filiform papillae are long and thin. Fungiform papillae contain taste buds, and filiform papillae have touch receptors that help the tongue move food around in the mouth. The filiform papillae create an abrasive surface that performs mechanically, much like a cat’s rough tongue that is used for grooming. Lingual glands in the lamina propria of the tongue secrete mucus and a watery serous fluid that contains the enzyme lingual lipase, which plays a minor role in breaking down triglycerides but does not begin working until it is activated in the stomach. A fold of mucous membrane on the underside of the tongue, the lingual frenulum, tethers the tongue to the floor of the mouth. People with the congenital anomaly ankyloglossia, also known by the non-medical term “tongue tie,” have a lingual frenulum that is too short or otherwise malformed. Severe ankyloglossia can impair speech and must be corrected with surgery.
The Salivary Glands
Many small salivary glands are housed within the mucous membranes of the mouth and tongue. These minor exocrine glands are constantly secreting saliva, either directly into the oral cavity or indirectly through ducts, even while you sleep. In fact, an average of 1 to 1.5 litres of saliva is secreted each day. Usually just enough saliva is present to moisten the mouth and teeth. Secretion increases when you eat, because saliva is essential to moisten food and initiate the chemical breakdown of carbohydrates. Small amounts of saliva are also secreted by the labial glands in the lips. In addition, the buccal glands in the cheeks, palatal glands in the palate, and lingual glands in the tongue help ensure that all areas of the mouth are supplied with adequate saliva.
The Major Salivary Glands
Outside the oral mucosa are three pairs of major salivary glands, which secrete the majority of saliva into ducts that open into the mouth:
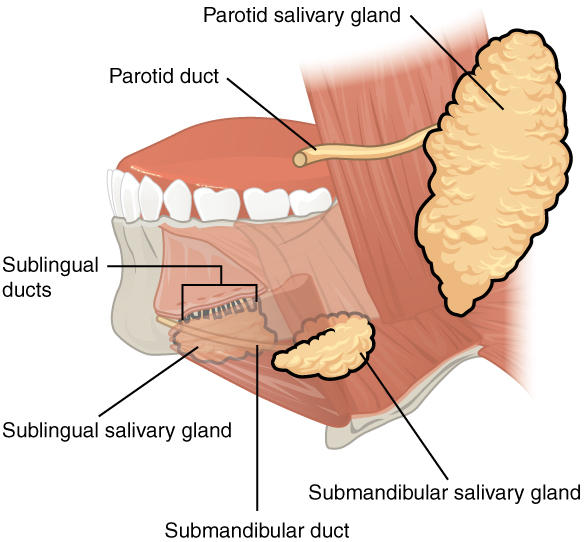
- The submandibular glands, which are in the floor of the mouth, secrete saliva into the mouth through the submandibular ducts.
- The sublingual glands, which lie below the tongue, use the lesser sublingual ducts to secrete saliva into the oral cavity.
- The parotid glands lie between the skin and the masseter muscle, near the ears. They secrete saliva into the mouth through the parotid duct, which is located near the second upper molar tooth (Figure 12.3.3).
Saliva
Saliva is essentially (95.5 percent) water. The remaining 4.5 percent is a complex mixture of ions, glycoproteins, enzymes, growth factors, and waste products. Perhaps the most important ingredient in salvia from the perspective of digestion is the enzyme salivary amylase, which initiates the breakdown of carbohydrates. Food does not spend enough time in the mouth to allow all the carbohydrates to break down, but salivary amylase continues acting until it is inactivated by stomach acids. Bicarbonate and phosphate ions function as chemical buffers, maintaining saliva at a pH between 6.35 and 6.85. Salivary mucus helps lubricate food, facilitating movement in the mouth, bolus formation, and swallowing. Saliva contains immunoglobulin A, which prevents microbes from penetrating the epithelium, and lysozyme, which makes saliva antimicrobial. Saliva also contains epidermal growth factor, which might have given rise to the adage “a mother’s kiss can heal a wound.”
Each of the major salivary glands secretes a unique formulation of saliva according to its cellular makeup, for example the parotid glands secrete a watery solution that contains salivary amylase. The submandibular glands have cells like those of the parotid glands, as well as mucus-secreting cells. Therefore, saliva secreted by the submandibular glands also contains amylase but in a liquid thickened with mucus. The sublingual glands contain mostly mucous cells, and they secrete the thickest saliva with the least amount of salivary amylase.
Homeostatic Imbalances
The Parotid Glands: Mumps
Infections of the nasal passages and pharynx can attack any salivary gland. The parotid glands are the usual site of infection with the virus that causes mumps (paramyxovirus). Mumps manifests by enlargement and inflammation of the parotid glands, causing a characteristic swelling between the ears and the jaw. Symptoms include fever and throat pain, which can be severe when swallowing acidic substances such as orange juice.
In about one-third of men who are past puberty, mumps also causes testicular inflammation, typically affecting only one testis and rarely resulting in sterility. With the increasing use and effectiveness of mumps vaccines, the incidence of mumps worldwide has decreased dramatically. Since the foundation of the vaccine in 1983, there have been no recorded childhood deaths due to mumps. Almost 95% of Australian toddlers (24 months old) were fully vaccinated against mumps in 2017, however the reported incidence rate has been gradually increasing in Australia. Majority of the outbreaks have been recorded in people 18-24 years of age, and it is speculated that this group missed their vaccination as children as they were born in a time when the disease rate was low. These outbreaks have been most commonly seen in the Aboriginal and Torres Straight Island populations.
Regulation of Salivation
The autonomic nervous system regulates salivation (the secretion of saliva). In the absence of food, parasympathetic stimulation keeps saliva flowing at just the right level for comfort as you speak, swallow, sleep, and generally go about life. Over-salivation can occur, for example, if you are stimulated by the smell of food, but that food is not available for you to eat. Drooling is an extreme instance of the overproduction of saliva. During times of stress, such as before speaking in public, sympathetic stimulation takes over, reducing salivation and producing the symptom of dry mouth often associated with anxiety. When you are dehydrated, salivation is reduced, causing the mouth to feel dry and prompting you to take action to quench your thirst.
Salivation can be stimulated by the sight, smell, and taste of food. It can even be stimulated by thinking about food. You might notice whether reading about food and salivation right now has had any effect on your production of saliva.
How does the salivation process work while you are eating? Food contains chemicals that stimulate taste receptors on the tongue, which send impulses to the superior and inferior salivatory nuclei in the brain stem. These two nuclei then send back parasympathetic impulses through fibres in the glossopharyngeal and facial nerves, which stimulate salivation. Even after you swallow food, salivation is increased to cleanse the mouth and to water down and neutralise any irritating chemical remnants, such as that hot sauce in your burrito. Most saliva is swallowed along with food and is reabsorbed, so that fluid is not lost.
The Teeth
The teeth, or dentes (singular = dens), are organs like bones that you use to tear, grind, and otherwise mechanically break down food.
Types of Teeth
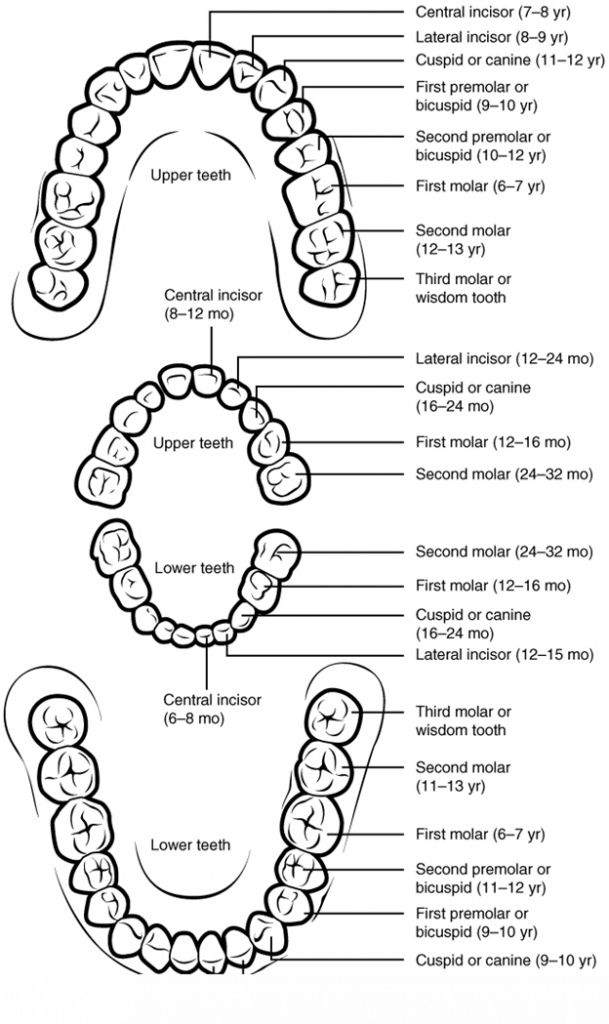
During the course of your lifetime, you have two sets of teeth (one set of teeth is a dentition). Your 20 deciduous teeth, or baby teeth, first begin to appear at about 6 months of age. Between approximately age 6 and 12, these teeth are replaced by 32 permanent teeth. Moving from the centre of the mouth toward the side, these are as follows (Figure 12.3.4):
- The eight incisors, four top and four bottom, are the sharp front teeth you use for biting into food.
- The four cuspids (or canines) flank the incisors and have a pointed edge (cusp) to tear up food. These fang-like teeth are superb for piercing tough or fleshy foods.
- Posterior to the cuspids are the eight premolars (or bicuspids), which have an overall flatter shape with two rounded cusps useful for mashing foods.
The most posterior and largest are the 12 molars, which have several pointed cusps used to crush food so it is ready for swallowing. The third members of each set of three molars, top and bottom, are commonly referred to as the wisdom teeth, because their eruption is commonly delayed until early adulthood. It is not uncommon for wisdom teeth to fail to erupt; that is, they remain impacted. In these cases, the teeth are typically removed by orthodontic surgery.
Anatomy of a Tooth
The teeth are secured in the alveolar processes (sockets) of the maxilla and the mandible, with this joint known as a gomphosis. Gingivae (commonly called the gums) are soft tissues that line the alveolar processes and surround the necks of the teeth. Teeth are also held in their sockets by a connective tissue called the periodontal ligament.
The two main parts of a tooth are the crown, which is the portion projecting above the gum line, and the root, which is embedded within the maxilla and mandible. Both parts contain an inner pulp cavity, containing loose connective tissue through which run nerves and blood vessels. The region of the pulp cavity that runs through the root of the tooth is called the root canal. Surrounding the pulp cavity is dentin, a bone-like tissue. In the root of each tooth, the dentin is covered by an even harder bone-like layer called cementum. In the crown of each tooth, the dentin is covered by an outer layer of enamel, the hardest substance in the body (Figure 12.3.5).
Although enamel protects the underlying dentin and pulp cavity, it is still nonetheless susceptible to mechanical and chemical erosion, or what is known as tooth decay. The most common form, dental caries (cavities) develops when colonies of bacteria feeding on sugars in the mouth release acids that cause soft tissue inflammation and degradation of the calcium crystals of the enamel. The digestive functions of the mouth are summarised in Table 12.3.1.
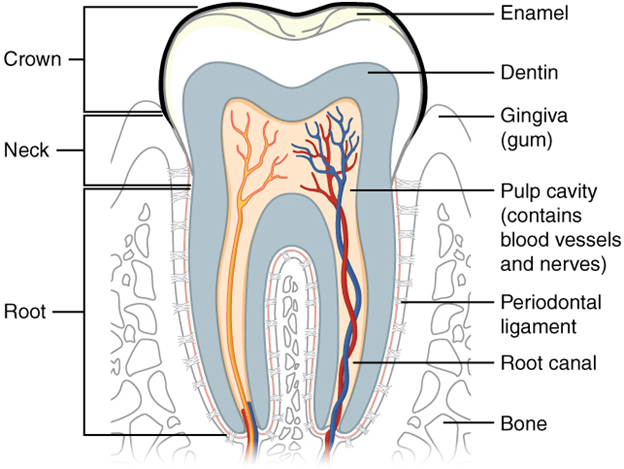
Table 12.3.1. Digestive Functions of the Mouth
| Structure | Action | Outcome |
| Lips and cheeks | Confine food between teeth |
|
| Salivary glands | Secrete saliva |
|
| Tongue’s extrinsic muscles | Move tongue sideways, and in and out |
|
| Tongue’s intrinsic muscles
|
Change tongue shape |
|
| Taste buds | Sense food in mouth and sense taste |
|
| Lingual glands | Secrete lingual lipase |
|
| Teeth | Shred and crush food |
|
The Pharynx
The pharynx (throat) is involved in both digestion and respiration. It receives food and air from the mouth, and air from the nasal cavities. When food enters the pharynx, involuntary muscle contractions close off the air passageways.
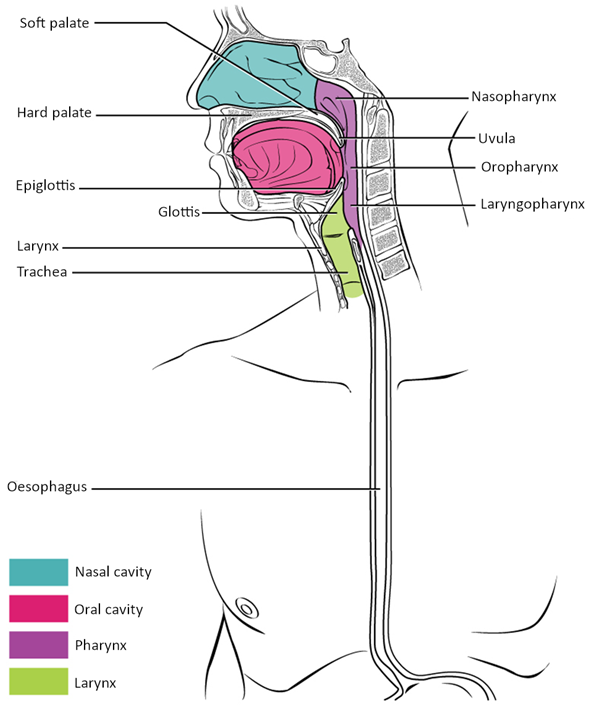
A short tube of skeletal muscle lined with a mucous membrane, the pharynx runs from the posterior oral and nasal cavities to the opening of the oesophagus and larynx. It has three subdivisions. The most superior, the nasopharynx, is involved only in breathing and speech. The other two subdivisions, the oropharynx and the laryngopharynx, are used for both breathing and digestion. The oropharynx begins inferior to the nasopharynx and is continuous below with the laryngopharynx (Figure 12.3.6). The inferior border of the laryngopharynx connects to the oesophagus, whereas the anterior portion connects to the larynx, allowing air to flow into the bronchial tree.
Histologically, the wall of the oropharynx is like that of the oral cavity. The mucosa includes a stratified squamous epithelium that is endowed with mucus-producing glands. During swallowing, the elevator skeletal muscles of the pharynx contract, raising and expanding the pharynx to receive the bolus of food. Once received, these muscles relax and the constrictor muscles of the pharynx contract, forcing the bolus into the oesophagus and initiating peristalsis.
Usually during swallowing, the soft palate and uvula rise reflexively to close off the entrance to the nasopharynx. At the same time, the larynx is pulled superiorly and the cartilaginous epiglottis, its most superior structure, folds inferiorly, covering the glottis (the opening to the larynx); this process effectively blocks access to the trachea and bronchi. When the food “goes down the wrong way,” it goes into the trachea. When food enters the trachea, the reaction is to cough, which usually forces the food up and out of the trachea, and back into the pharynx.
The Oesophagus
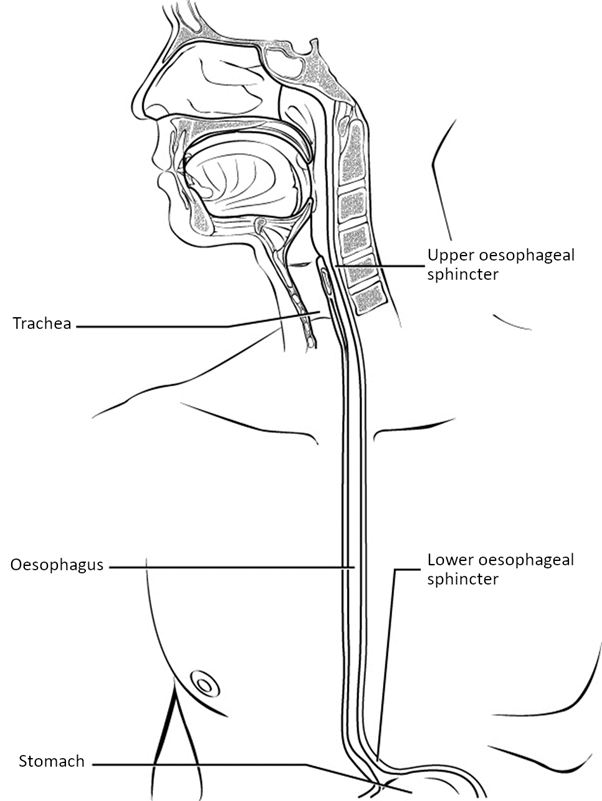
The oesophagus is a muscular tube that connects the pharynx to the stomach. It is approximately 25.4 cm in length, located posterior to the trachea, and remains in a collapsed form when not engaged in swallowing. As you can see in Figure 12.3.7, the oesophagus runs a mainly straight route through the mediastinum of the thorax. To enter the abdomen, the oesophagus penetrates the diaphragm through an opening called the oesophagus hiatus.
Passage of Food Through the Oesophagus
The upper oesophagus sphincter, which is continuous with the inferior pharyngeal constrictor, controls the movement of food from the pharynx into the oesophagus. The upper two-thirds of the oesophagus consists of both smooth and skeletal muscle fibres, with the latter fading out in the bottom third of the oesophagus. Rhythmic waves of peristalsis, which begin in the upper oesophagus, propel the bolus of food toward the stomach. Meanwhile, secretions from the oesophageal mucosa lubricate the oesophagus and food. Food passes from the oesophagus into the stomach at the lower oesophageal sphincter (also called the gastroesophageal or cardiac sphincter). Recall that sphincters are muscles that surround tubes and serve as valves, closing the tube when the sphincters contract and opening it when they relax. The lower oesophageal sphincter relaxes to let food pass into the stomach, and then contracts to prevent stomach acids from backing up into the oesophagus. Surrounding this sphincter is the muscular diaphragm, which helps close off the sphincter when no food is being swallowed. When the lower oesophageal sphincter does not completely close, the stomach’s contents can reflux (that is, back up into the oesophagus), causing heartburn or gastroesophageal reflux disease (GERD).
Histology of the Oesophagus
The mucosa of the oesophagus is made up of an epithelial lining that contains non-keratinised, stratified squamous epithelium, with a layer of basal and parabasal cells. This epithelium protects against erosion from food particles. The mucosa’s lamina propria contains mucus-secreting glands. The muscularis layer changes according to location: In the upper third of the oesophagus, the muscularis is skeletal muscle. In the middle third, it is both skeletal and smooth muscle. In the lower third, it is smooth muscle. As mentioned previously, the most superficial layer of the oesophagus is called the adventitia, not the serosa. In contrast to the stomach and intestines, the loose connective tissue of the adventitia is not covered by a fold of visceral peritoneum. The digestive functions of the oesophagus are identified in Table 12.3.2.
Table 12.3.2. Digestive Functions of the Oesophagus
| Action | Outcome |
| Upper oesophageal
sphincter relaxation
|
Allows the bolus to move from the laryngopharynx to the oesophagus |
| Peristalsis
|
Propels the bolus through the oesophagus |
| Lower oesophageal sphincter relaxation
|
Allows the bolus to move from the oesophagus into the stomach and prevents chime from entering the oesophagus |
| Mucus secretion | Lubricates the oesophagus, allowing easy passage of the bolus |
Deglutition
Deglutition is another word for swallowing—the movement of food from the mouth to the stomach. The entire process takes about four to eight seconds for solid or semisolid food, and about one second for very soft food and liquids. Although this sounds quick and effortless, deglutition is, in fact, a complex process that involves both the skeletal muscle of the tongue and the muscles of the pharynx and oesophagus. It is aided by the presence of mucus and saliva. There are three stages in deglutition: the voluntary phase, the pharyngeal phase and the oesophageal phase (Figure 12.3.8). The autonomic nervous system controls the latter two phases.
The Voluntary Phase
The voluntary phase of deglutition (also known as the oral or buccal phase) is so called because you can control when you swallow food. In this phase, chewing has been completed and swallowing is set in motion. The tongue moves upward and backward against the palate, pushing the bolus to the back of the oral cavity and into the oropharynx. Other muscles keep the mouth closed and prevent food from falling out. At this point, the two involuntary phases of swallowing begin.
The Pharyngeal Phase
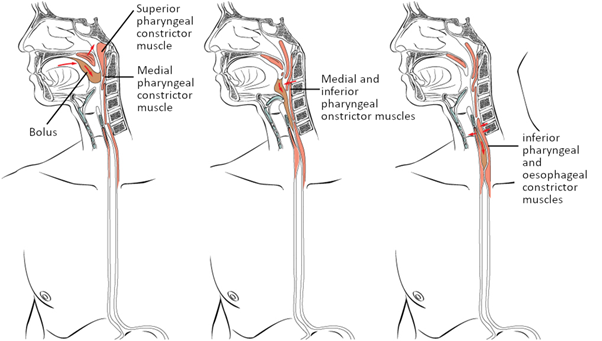
In the pharyngeal phase, stimulation of receptors in the oropharynx sends impulses to the deglutition centre (a collection of neurons that controls swallowing) in the medulla oblongata. Impulses are then sent back to the uvula and soft palate, causing them to move upward and close off the nasopharynx. The laryngeal muscles also constrict to prevent aspiration of food into the trachea. At this point, deglutition apnoea takes place, which means that breathing ceases for a very brief time. Contractions of the pharyngeal constrictor muscles move the bolus through the oropharynx and laryngopharynx. Relaxation of the upper oesophageal sphincter then allows food to enter the oesophagus.
The Oesophageal Phase
The entry of food into the oesophagus marks the beginning of the oesophageal phase of deglutition and the initiation of peristalsis. As in the previous phase, the complex neuromuscular actions are controlled by the medulla oblongata. Peristalsis propels the bolus through the oesophagus and toward the stomach. The circular muscle layer of the muscularis contracts, pinching the oesophageal wall and forcing the bolus forward. At the same time, the longitudinal muscle layer of the muscularis also contracts, shortening this area and pushing out its walls to receive the bolus. In this way, a series of contractions keeps moving food toward the stomach. When the bolus nears the stomach, distention of the oesophagus initiates a short reflex relaxation of the lower oesophageal sphincter that allows the bolus to pass into the stomach. During the oesophageal phase, oesophageal glands secrete mucus that lubricates the bolus and minimises friction.
Section Review
In the mouth, the tongue and the teeth begin mechanical digestion, and saliva begins chemical digestion. The pharynx, which plays roles in breathing and vocalisation as well as digestion, runs from the nasal and oral cavities superiorly to the oesophagus inferiorly (for digestion) and to the larynx anteriorly (for respiration). During deglutition (swallowing), the soft palate rises to close off the nasopharynx, the larynx elevates, and the epiglottis folds over the glottis. The oesophagus includes an upper oesophageal sphincter made of skeletal muscle, which regulates the movement of food from the pharynx to the oesophagus. It also has a lower oesophageal sphincter, made of smooth muscle, which controls the passage of food from the oesophagus to the stomach. Cells in the oesophageal wall secrete mucus that eases the passage of the food bolus.
Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
